

Key Points
- Multiple myeloma (MM) is a complex, heterogenous, continuously evolving disease that requires personalized and multidisciplinary approaches to treatment.
- Disease presentation, patient fitness, and the presence of high-risk genetic features are crucial factors to making treatment decisions in MM.
- MM is an active area of clinical research, and new immunotherapies are being investigated and integrated into the standard of care.
MM is a complex and heterogeneous malignant disease that exhibits a wide spectrum of clinical and molecular characteristics. Presenting features such as the stage of disease, cytogenetic abnormalities, presence of bone lesions, renal function, patient’s age, and overall health status form a complex clinical mosaic. There is no single molecular abnormality to target but rather a constellation of molecular abnormalities, leading to a molecular background that changes spatially (within the bone marrow and in extramedullary sites) and, in time as the disease evolves, within a changing/weakening host immune environment. As a result, MM cells are a moving target, requiring continual treatment adjustments. Despite advanced diagnostic tools and molecular profiling technologies, we are lacking relevant molecularly targeted therapies. Exceptions include the unique activity of BCL-2 inhibitors in patients harboring t(11;14), as well as limited success with BRAF/MEK inhibition. On the other hand, we have very active immunotherapies targeting phenotypic characteristics of the clone (eg, surface antigens CD38, BCMA, GPRC5D, FcRH5, and SLAMF7).
Considerations When Determining Treatment Type
Disease presentation is critical to treatment decisions. Patients with asymptomatic (“smoldering”) myeloma do not require immediate therapy; however, treating earlier rather than later may be associated with better outcomes for “high-risk” asymptomatic MM, which can be identified with more “personalized” risk scores.1 There are 2 different approaches to the treatment of high-risk asymptomatic MM: (1) using mild, oral, fixed-duration therapy (eg, lenalidomide/dexamethasone or lenalidomide alone) that aims to delay progression to symptomatic disease and prolong survival, and (2) using aggressive, triple/quadruple combinations with high-dose therapy followed by fixed-duration maintenance, aiming to cure the disease.2-4 Currently, randomized clinical trials support the first approach, but data are insufficient for the more aggressive one. Ongoing prospective randomized trials will enable more personalized decision-making.
Patients with symptomatic disease should start therapy to avoid further complications. Certain presenting features may require more aggressive approaches, but comorbidities and the patient’s frailty significantly influence treatment decisions. Comprehensive geriatric assessment, beyond the typical assessment of fitness level with performance status scales, may offer a clinically relevant approach to personalized therapy, leading to regimen, dose, and schedule adaptations.5 Early treatment discontinuation because of toxicity is associated with poorer outcomes, and a “do-no-harm” approach becomes critical to improve quality of life and prolong survival. Patients presenting with severe renal impairment (RI) require special supportive care and the administration of non-nephrotoxic, rapidly acting and effective therapy such as combinations of proteasome inhibitors (preferably bortezomib because of its better safety profile in the context of RI) with anti-CD38 monoclonal antibodies, as well as dexamethasone and an immunomodulatory drug or cyclophosphamide.6 Management of hypercalcemia and bone pain in those with RI may require the use of denosumab instead of zoledronate because of its better renal toxicity profile. Patients presenting with extensive bone disease or severe bone pain and disability, or those at imminent risk of fractures or spinal cord compression, require anti–bone resorption agents on top of effective, rapidly acting therapy and multidisciplinary treatment. Consultation with orthopedic surgeons is advised, as well as radiotherapy in selected cases, given that most skeletal events occur early after starting therapy.7
Disease presenting with high-risk genetic features requires an aggressive approach. Patients with high-risk disease are identified by the presence of certain cytogenetic abnormalities, such as the following: deletion 17p or specific chromosome 14 translocations [t(4;14) and t(14;16)]; the concurrent presence of amplification/addition of 1q21 or high-risk molecular scores with high–tumor burden (ie, stage III of the International Staging System) disease and/or elevated levels of serum LDH, hypercalcemia, plasma cell leukemia or plasma cell leukemia–like features; and high numbers of peripheral blood circulating clonal plasma cells.8-11 Patients with high-risk disease may benefit from achieving deep responses and reaching the level of undetectable minimal residual disease (MRD). Intensive, multiagent regimens, which include drugs with different mechanisms of action, consolidation with high-dose melphalan, and more intensive maintenance than in conventional approaches, increase rates of sustained undetectable MRD.
Unpacking the Data
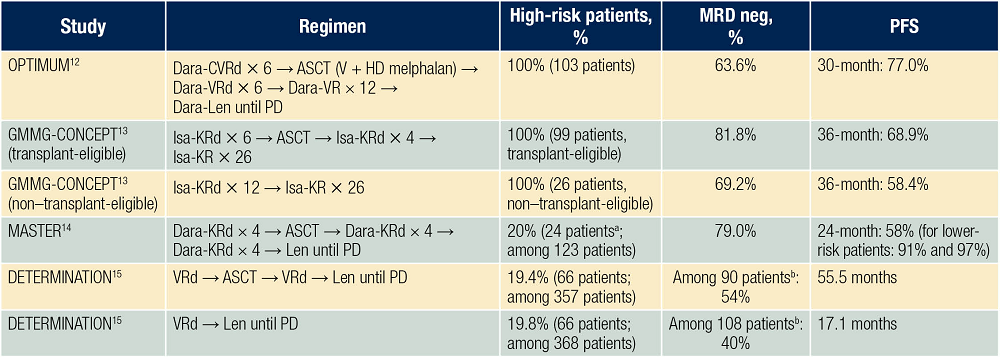
The OPTIMUM/MUK IX trial used a quintuplet induction (daratumumab, cyclophosphamide, bortezomib, lenalidomide, and dexamethasone) in patients with high-risk newly diagnosed MM, resulting in high MRD-negativity rates (63.6%) after autologous stem cell transplant (ASCT) and a 30-month progression-free survival (PFS) rate of 77% (Table 112-15). In the GMMG-CONCEPT trial, induction included the quadruplet of isatuximab, carfilzomib, lenalidomide, and dexamethasone, and, after ASCT and consolidation, 67.7% of patients achieved MRD negativity, 81.8% reached MRD negativity at any time point, and MRD negativity was sustained for at least 1 year in 62.6% of patients; the median PFS was not reached after 44 months of follow-up.13 In the MASTER trial, induction with a quadruplet (daratumumab, carfilzomib, lenalidomide, and dexamethasone [Dara-KRd]), consolidation with ASCT, and further consolidation with Dara-KRd, adapted to the presence of MRD, were given. In patients with low-risk disease, shorter consolidation was associated with low recurrence risk, but not in patients with high-risk disease, despite similar MRD-negative rates; sustainability of undetectable MRD seems to be the key target for patients at high risk.14 Ongoing trials (eg, PERSEUS) will define the role of adapted consolidation and maintenance based on MRD status, providing a personalized, response-adapted approach to therapy.16 The above studies have included intensive induction, consolidation, and maintenance, being suitable for fitter patients. However, even without ASCT, 4-drug regimens (as in the GMMG-CONCEPT trial) can also improve outcomes for high-risk, non–transplant-eligible patients.
Immunotherapy Causes a Paradigm Shift in the Treatment Landscape
Novel immunotherapies are being rapidly implemented into treatment algorithms, bringing about a paradigm shift in myeloma therapy. These therapies capitalize on the immune system’s ability to recognize and eliminate cancer cells; the landscape and fitness of the immune system becomes a critical factor to their success.17 Cellular and T-cell–engaging therapies are being explored as part of early therapy in patients with high-risk disease and could further improve MRD sustainability, either as part of induction consolidation or as part of maintenance. There is a continuous search to identify biomarkers that would allow us to choose between different immunotherapies and relevant targets on MM cells (eg, BCMA, GPRC5d, FcRH5, SLAMF7, CD38). The optimal sequence of immunotherapies, immune system fitness, patient fitness and comorbidities, and logistics and costs form a complex foundation on which to build personalized treatments.
Patients with less aggressive disease (ie, “standard risk”) may be candidates for less intense regimens or fixed-duration maintenance. In the DETERMINATION study, consolidation with ASCT improved PFS over non-ASCT, but there was no difference in the overall survival, especially among patients at standard risk when maintenance until progression was used.15 Defining “standard risk” is not always straightforward; even among patients with the above characteristics, a minority will relapse relatively early, being refractory to key drugs. Risk of early relapse is significantly higher in high-risk myeloma, but early relapse after or during an active therapy defines a “functionally high-risk” group with dismal prognosis when conventional approaches are used. New combination regimens, novel immunotherapies, and cellular therapies improve disease management, and this group of patients could benefit from personalized approaches that target the unique biology of the disease that escaped therapy early on its course.18
Providing the “right treatment to the right patient at the right time” is a dynamic and evolving process, and there is still a lot of ground to cover. We have just made the first steps; the future holds great promise.
References
- Cowan A, Ferrari F, Freeman SS, et al. Personalised progression prediction in patients with monoclonal gammopathy of undetermined significance or smouldering multiple myeloma (PANGEA): a retrospective, multicohort study. Lancet Haematol. 2023;10(3):e203-e212.
- Mateos M-V, Hernández M-T, Giraldo P, et al. Lenalidomide plus dexamethasone for high-risk smoldering multiple myeloma. N Engl J Med. 2013;369(5):438-447.
- Lonial S, Jacobus S, Fonseca R, et al. Randomized trial of lenalidomide versus observation in smoldering multiple myeloma. J Clin Oncol. 2020;38(11):1126-1137.
- Kazandjian D, Hill E, Dew A, et al. Carfilzomib, lenalidomide, and dexamethasone followed by lenalidomide maintenance for prevention of symptomatic multiple myeloma in patients with high-risk smoldering myeloma: a phase 2 nonrandomized controlled trial. JAMA Oncol. 2021;7(11):1678-1685.
- Larocca A, Palumbo A. Optimizing treatment for elderly patients with newly diagnosed multiple myeloma: a personalized approach. J Clin Oncol. 2016;34(30):3600-3604.
- Dimopoulos MA, Merlini G, Bridoux F, et al; International Myeloma Working Group. Management of multiple myeloma-related renal impairment: recommendations from the International Myeloma Working Group. Lancet Oncol. 2023;24(7):e293-e311.
- Raje N, Terpos E, Willenbacher W, et al. Denosumab versus zoledronic acid in bone disease treatment of newly diagnosed multiple myeloma: an international, double-blind, double-dummy, randomised, controlled, phase 3 study. Lancet Oncol. 2018;19(3):370-381.
- D’Agostino M, Cairns DA, Lahuerta JJ, et al. Second Revision of the International Staging System (R2-ISS) for overall survival in multiple myeloma: a European Myeloma Network (EMN) report within the HARMONY project. J Clin Oncol. 2022;40(29):3406-3418.
- Hofste Op Bruinink D, Kuiper R, van Duin M, et al. Identification of high-risk multiple myeloma with a plasma cell leukemia-like transcriptomic profile. J Clin Oncol. 2022;40(27):3132-3150.
- Jelinek T, Bezdekova R, Zihala D, et al. More than 2% of circulating tumor plasma cells defines plasma cell leukemia-like multiple myeloma. J Clin Oncol. 2023;41(7):1383-1392.
- Kostopoulos IV, Ntanasis-Stathopoulos I, Rousakis P, et al. Circulating plasma cells in newly diagnosed multiple myeloma: prognostic and more. J Clin Oncol. 2023;41(3):708-710.
- Kaiser MF, Hall A, Walker K, et al. Daratumumab, cyclophosphamide, bortezomib, lenalidomide, and dexamethasone as induction and extended consolidation improves outcome in ultra-high-risk multiple myeloma. J Clin Oncol. 2023;41(23):3945-3955.
- Leypoldt LB, Besemer B, Asemissen AM, et al. Isatuximab, carfilzomib, lenalidomide, and dexamethasone (Isa-KRd) in front-line treatment of high-risk multiple myeloma: interim analysis of the GMMG-CONCEPT trial. Leukemia. 2022;36(3):885-888.
- Costa LJ, Chhabra S, Medvedova E, et al. Daratumumab, carfilzomib, lenalidomide, and dexamethasone with minimal residual disease response-adapted therapy in newly diagnosed multiple myeloma. J Clin Oncol. 2022;40(25):2901-2912.
- Richardson PG, Jacobus SJ, Weller EA, et al; DETERMINATION Investigators. Triplet therapy, transplantation, and maintenance until progression in myeloma. N Engl J Med. 2022;387(2):132-147.
- Sonneveld P, Broijl A, Gay F, et al. Bortezomib, lenalidomide, and dexamethasone (VRd) ± daratumumab (DARA) in patients (pts) with transplant-eligible (TE) newly diagnosed multiple myeloma (NDMM): A multicenter, randomized, phase III study (PERSEUS). J Clin Oncol. 2019;37:15s (suppl; abstr TPS8055).
- Friedrich MJ, Neri P, Kehl N, et al. The pre-existing T cell landscape determines the response to bispecific T cell engagers in multiple myeloma patients. Cancer Cell. 2023;41(4):711-725.e6.
- Poos AM, Prokoph N, Przybilla MJ, et al. Resolving therapy resistance mechanisms in multiple myeloma by multi-omics subclone analysis. Blood. 2023;142(19):1633-1646.
See also: https://dailynews.ascopubs.org/do/understanding-personalized-treatment-approaches-multiple-myeloma

{kind=link}